Which Herbal Therapies Can Be Recommended to a Client With Breast Pain? Select All That Apply.
![]() Open access peer-reviewed affiliate
Open access peer-reviewed affiliate
Herbal Remedies for Breast Cancer Prevention and Treatment
Submitted: May 6th, 2019 Reviewed: September 11th, 2019 Published: March 25th, 2020
DOI: 10.5772/intechopen.89669

IntechOpen Downloads
1,571
Full Chapter Downloads on intechopen.com
![]()
Altmetric score
Overall attention for this chapters
Abstract
Chest cancer is amongst the most common type of cancer in women around the globe. Prevention of breast cancer is better than its treatment. Considering of the molecular variation and complexity underlying breast cancer occurrence, its treatment past using chemotherapy and/or radiotherapy is very complicated and often leads to undesirable side effects. Plants and their extracts accept been used for centuries for the handling of almost every disease and breast cancer is non an exception. Herbal products can be trusted for cancer treatment because of their low toxicity. Also, herbal remedies are hands accustomed by the majority of adult female suffering from breast cancer because of their piece of cake availability and affordability. In the last decade, a large number of plants and their compounds were reported to evidence promising anticancerous effects against breast cancer cells in both in vivo and in vitro models. However, their beneficial effects on breast cancer treatment are still hundred-to-one due to the lack of randomized clinical trials. This chapter is defended to reporting the potential of some herbal products for the prevention and/or treatment of chest cancer. Besides, it focused on the anticarcinogenic mechanism of those phytocompounds to study their potential chemotherapeutic role.
Keywords
- herbal remedies
- phytochemicals
- phytoestrogens
- chest cancer
*Address all correspondence to: pbmazumder65@gmail.com
i. Introduction
According to Earth Health Organization (WHO), cancer is the second leading cause of death later on cardiovascular diseases and a growing health event globally. Breast cancer is the almost usually diagnosed type of cancer amid females bookkeeping for approximately i-quarter of cancers in females globally. Neat research efforts are in place to understand the cause of breast cancer onset, to identify the critical molecular mechanism of its progression, and to define new ways of treating it with lower and limited toxicity. These efforts are certainly encouraging since overall survival has greatly improved in several chest cancer types during the last decade. Since 1990, bloodshed rates of chest cancer have reduced significantly by 25%, this is at least in role due to the significant improvement in its treatment [one]. Handling of cancer mainly relies on chemotherapy that uses cytotoxic agents for killing cancer cells. However, these agents or drugs affect both cancer cells every bit well as salubrious cells, causing an array of side effects during the therapy or afterwards the therapy. To overcome these problems, electric current research is emphasized to explore herbal remedies that selectively targets cancer cells. Too this, unlike other cancer types, breast cancer has diverse genetic mutations that affect several pathways [two]. These complexities assistance to distinct pathological types with different clinical outcomes [three]. Therefore, response to a certain chemotherapeutic drug may differ in dissimilar patients and lack of proper treatment plan may increment the toxicity furthermore. One of the encouraging approaches to overcome drug toxicity is to await for culling medicines that have less or selective toxicity toward cancer cells [four]. In recent years, many studies accept demonstrated selective cytotoxicity of a variety of herbal compounds that can be used as potential chemotherapeutics [4]. Meanwhile, diverse herbal products were reported to forbid and/or palliate the side furnishings of treatment, improve quality of life, and reduce stress. However, the usefulness of herbal remedies for chest cancer prevention and/or treatment is nonetheless ambiguous due to the lack of randomized clinical trials. These objectives will exist achievable only if the herbal compounds that showed promising anticancer action tin can be successfully transferred to clinical trials.
Advertisement
2. Current scenario and future burden of chest cancer
Cancer of the chest is amidst the most oftentimes diagnosed cancer and the leading crusade of cancer-related deaths in females globally. According to International Agency for Research on Cancer (IARC's) Globocan information on 2018, chest cancer acquired 0.62 million deaths in 2022 and another ii.08 million new cases were identified, which is xi.vi% of all cancer types recorded [5]. At the current rate, the number of incident cases is expected to rise to three.05 one thousand thousand, and the bloodshed troll is expected to ascent to a nervus-racking half dozen.99 million by 2040 [6]. Approximately 1 in ten women is diagnosed with chest cancer at some time in their lives [3].
Epidemiological ascertainment shows that the incidence of breast cancer is continuously raising in both industrialized and developing countries [vii]. Breast cancer is a disease largely triggered by environmental and lifestyle factors than genetic, which is believed to be responsible for only ten–15% of all breast cancer cases [8]. Various gamble factors like age (>50), family unit history of chest cancer, woman's reproductive history such equally early on menarche, nulliparity or belatedly pregnancy, and belatedly menopause mainly help to breast cancer onset [ix]. In addition, prolonged use of oral contraceptive and hormone replacement therapy are too known risk factors of this disease among postmenopausal women [10].
Advertisement
three. Molecular feature of breast cancer occurrence, progression, and treatment
The onset of cancer is a event of several sequential molecular events. Virtually common of them is a mutation in a Deoxyribonucleic acid molecule that codes for a poly peptide that either triggers cell division, proliferation, and growth or that signals termination of all these molecular events [11]. Therefore, harm to DNA or a protein that regulates cell cycle may atomic number 82 to uncontrolled division and growth of cells, the condition is cancer. It is a hyperproliferative disease that involves molecular amending resulting in apoptosis dysregulation, proliferation, angiogenesis, and metastasis [12].
Chest cancer is one of the commonest types of cancer and characterized by distinct pathological types with different clinical outcomes. It has unlike stages that ascend from ductal hyperproliferation, which changes into ductal carcinoma
Chest cancer therapeutics include drugs that protect genomic stability by preventing Deoxyribonucleic acid damage, inhibit the cell cycle by disrupting cellular integrity or by inducing apoptotic cell death, and cake certain pathways that are responsible for abnormal cell growth (Table 1). Majority of chest cancer cases express the estrogen hormone receptor, which helps the cancer cells to proliferate chop-chop by the growth-promoting effects of circulatory estrogens [17]. Therefore, current therapies are targeted at abrogating estrogen dependence for estrogen receptor (ER)-positive chest cancers [17]. One of the successful and efficient approaches is the employment of a selective estrogen receptor modulator (SERM) similar tamoxifen, which binds to the ER that induces a conformational change in the receptor resulting in obstruction of estrogenic expression [18, xix]. Even so, tamoxifen like SERMs exhibits many notable side effects including—secondary cancer, cardiovascular diseases past their estrogenic activity in other tissues and organs. The efficiency of tamoxifen is challenged by the evolution of highly potent third-generation aromatase inhibitors (AIs) that represents a promising approach in endocrine therapy of breast cancer [20]. The aromatase inhibitor drugs like anastrozole and letrozole reduce estrogen product by competitive inhibition of the enzyme aromatase, although the long-term wellness furnishings of AIs are doubtful [21]. Another effective strategy in breast cancer treatment is the implementation of a growth factor inhibitor. 1 of the offset identified targets of these growth inhibitors was the epidermal growth factor receptor (EGFR) that plays a vital role in the survival of cancer cells and developing multidrug resistance [22]. The effectiveness of the small-scale molecule EGFR tyrosine kinase inhibitor similar gefitinib is highly appreciated for the treatment of breast cancer; notwithstanding, information technology failed to produce notable comeback in advance stages of chest cancer [23].
Table one.
Commonly used chest cancer chemotherapeutic drugs, their targets, and mechanism of action [26].
Approximately 20% of breast cancer cases show overexpression of the HER2 that results in aggressive affliction and reduced survival [17]. In nowadays, trastuzumab and lapatinib are the only marketed drugs used to inhibit the HER2-mediated growth and proliferation signaling [17]. Other than this, enzyme-mediated Deoxyribonucleic acid impairment is an effective approach used in cancer chemotherapy. Doxorubicin, an anthracycline drug, binds with Deoxyribonucleic acid by intercalation with base pairs, which results in an elevated level of DNA-topoisomerase Ii covalent complexes inhibiting topoisomerase II activity [24]. Other anticancer drugs inhibit mitosis by interrupting the microtubule stability, hence blocking the transition from metaphase to anaphase [25]. Subsequently, the cell undergoes mitotic abort or programmed cell death (apoptosis). For instance, vincristine and vinorelbine inhibit the polymerization of microtubules past binding to either the vinca domain or taxoid-binding domain that interferes between β- and α-subunit of tubulin [25]. On the other manus, microtubule-stabilizing drugs similar paclitaxel hyperstabilizes the microtubule assembly past binding to the inner surface of the microtubule at a taxoid-binding site on β-tubulin resulting in mitotic arrest in the cell [25]. All these strategies helped in reducing bloodshed due to breast cancer and increased the survival charge per unit; withal, they appear with certain side furnishings that may be either low and brusk term or loftier and life threatening.
Advert
four. Chemotherapeutic-associated toxicity in breast cancer handling
The role of chemotherapy in curing cancer is even so doubtful [27]. Fifty-fifty information technology decreases the risk of recurrence and helps the patient to live longer with improved quality of life in case of metastatic chest cancer. But its use associated with sure risk factors or side effects—some of the side effects are short term and modest, whereas others may get more than serious and life threatening [27]. Table 2 describes a few usually used chemotherapeutic drugs and their side effects.
Table 2.
Oft used chemotherapeutic drugs in chest cancer treatment and their common side effects associated with them [26, 28, 29, thirty].
Amidst the most common side effects of chemotherapeutic drugs is its nonselective toxicity, where it destroys the normal body cells such equally those in the hair follicle, bone marrow, and cells of other important organs along with the cancer cells. Quite a few chemotherapeutic drugs affect the nervus endings or synaptic gaps in hands and feet that may result into numbness, pain, burning or tingling, sensitivity to cold or heat, or weakness in your extremities [31]. Too, chemotherapeutic drugs may severely impairment the immune cells as wells equally the brain cells, making the patient vulnerable to infectious diseases and impaired cognitive functions [32]. These side furnishings may exist temporary and may disappear after a few months of completion of chemotherapy. Other disquisitional side effects that arise due to sure chemotherapeutic drugs may last longer—infertility is one of them [33]. Chemotherapeutics that impairment ovaries may lead to menopause symptoms, similar hot flashes and vaginal dryness, where menstrual bicycle becomes irregular or permanently ceases making pregnancy impossible [34]. Farther, early on menopause in premenopausal women due to the employ of aromatase inhibitor agents in adjuvant therapy causes a hypoestrogenic condition that negatively impacts bone density resulting in osteopenia or osteoporosis [35].
Likewise, long-term chemotherapeutic toxicity results in cardiac diseases and may trigger secondary cancer such as marrow neoplasm or leukemia [36, 37]. Chemotherapy-linked cardiotoxicity is another major setback of cancer therapy that increases the mortality rate because of the loftier prevalence of cardiovascular diseases in cancer patients [38]. The cardiotoxicity leads to congestive middle failure (CHF), which is more than prevalence in young and elderly patients. It has been reported that the breast cancer patients aged between 65 and 70 years, who received adjuvant anthracycline chemotherapy, had significantly higher rates of CHF [39]. In another investigation, a widely used chemotherapeutic drug, doxorubicin, was reported to cause CHF in worryingly 26% of the patients suffering from breast carcinoma [40, 41]. Additionally, it was observed that 0.5% of chest cancer patients adult different types of marrow neoplasm (MN) or leukemia later on a few years of chemotherapy [42]. The take a chance of developing MN is higher in the first few years after chemotherapy. Furthermore, chemotherapeutic drugs may also disrupt the normal psychological land of patients in certain cases [43, 44].
The side effects that arise due the conventional chemotherapy is mainly due to lack of specificity of the drugs for cancer cells. Majority of the widely used chemotherapeutic drugs causes agin damage to normal cells and key organs, which limits the dose of a drug that tin can be used [45]. This explains the reason why cancer drugs have a low therapeutic index. Several approaches are being considered to address this result in order to amend the effectiveness of anticancer drugs. One of the popular approaches among them is searching for natural compounds that inhibit cancer jail cell growth without disrupting the functioning of healthy cells.
Advertizing
5. Ethnomedicine and herbal compounds used for cancer handling
Plants accept played a cardinal role in the survival and evolution of human beings as they accept provided the basic need of mankind like food, wearable, shelter, and medicine since the beginning of the man race. Plants have formed the footing of traditional medicine systems like Ayurveda, Unani, and Chinese traditional medicines that have served mankind with their health needs. A larger part of the population in developing and underdeveloped countries relies on herbal medicine for solving treating their principal health issues. Traditional herbal medicines become popular because of their cost-effectiveness, abundancy, and less or no side effects. In contempo years, global emphasis on plant research has increased to detect out drug-like substances from traditionally used medicinal plants. Moreover, several naturally occurring establish-based compounds like curcumin, resveratrol, quercetin, and many more showed promising anticancerous furnishings and are gaining involvement as an adjuvant chemotherapeutic agent. Likewise, naturally occurring compounds cause less toxicity to healthy cells and in sure cases testify selective toxicity against abnormal or diseased cells [46]. This might be the reason that today a large number of drugs being marketed are structurally like to the structure of naturally occurring compounds.
Herbal compounds prove a variety of anticancer activity mainly antioxidant, anti-inflammatory, antimutagenic, and apoptosis-inducing activeness that may help prevent cancer evolution in the early stage (Figure one). Dietary consumption of acceptable quantity of these herbal products may assistance in prevention and treatment of breast cancer by jail cell bike arrest, induction of apoptosis, regulating carcinogen metabolism and oncogenic expression, inhibiting cell adhesion, proliferation and migration, and blocking signaling pathways that are essential for cancer progression [47].

Effigy one.
Features of herbal compounds that aspect to their anticancer activity.
Between the year 1981 and 2014, 136 anticancer drugs were brought to utilize around the globe, about 83% of which were either herbal compounds or their derivatives [48]. A number of anticancer drugs have already in use for the treatment of breast cancer—including vincristine, vinblastine, paclitaxel, and docetaxel [49]. Despite the success of herbal products in curing breast cancer and its associated complexities, not many herbal products are making through preclinical or clinical trials. Hence, greater try is necessary to successfully transfer these agents to an ideal clinical setting to assess their potential for herbal therapies.
Advertisement
6. Herbal products used for prevention of breast cancer
Breast cancer is a preventable disease [50]. Estrogens play a major function in promoting the proliferation of normal breast cells besides as neoplastic chest epithelium [51]. Almost xl–70% of breast cancers are estrogen receptor positive [52]. Hence, blocking the estrogen receptor for the treatment and chemoprevention of breast cancer is ane of the significant approaches. Plant-based estrogen-like compounds or phytoestrogens were originally proposed equally cancer-protective agents. This claim was strongly supported by an epidemiological study that revealed a low breast cancer incidence in the soy-consuming population [53, 54]. Phytoestrogens are structural analogues of the mammalian hormone, estrogen, and thus can bind weakly to the hormone receptor [55]. Structurally, phytoestrogen can be grouped into flavones, flavanones, lignans, coumestans, and stilbenes [56]. The structure of important members of different classes of phytoestrogens is given in Figure 2. Soybean and soy product is a rich source of isoflavones [57]. Other phytoestrogen classes are legumes and lignans found in seeds, nuts, whole grains, fruit, and vegetables [57]. Historically, the rate of breast cancer occurrence in the U.s. is 4–7 times college than that of Asian population where the consumption of dietary isoflavones is comparatively as college as twenty to lxxx mg/d [58]. In improver, epidemiological observations also revealed a modest 30% reduction in chest cancer risk for women with a higher pct of dietary lignan intake [57]. Therefore, consumption of phytoestrogen-rich nutrition is one of the many potential protective lifestyles against breast cancer. Recently, there are increasing pieces of evidence that phytoestrogen activity inhibits key steroidogenic enzymes activity involved in the synthesis of estradiol from circulating androgens and estrogen sulfate [7]. Consequently, this activity could play a major part in protection against breast cancer. Besides inhibiting the estrogenic activity, phytoestrogens were likewise reported to actuate the G-protein coupled receptor, GPR30 or GPER-1, described as a novel estrogen receptor and play a pregnant role in estrogen-dependent diseases like breast cancer [59]. Nevertheless, the action of phytoestrogens is unclear and depends on more than than one factors that include—its construction, metabolism, its relative availability compared to that of endogenous estrogen [60, 57].
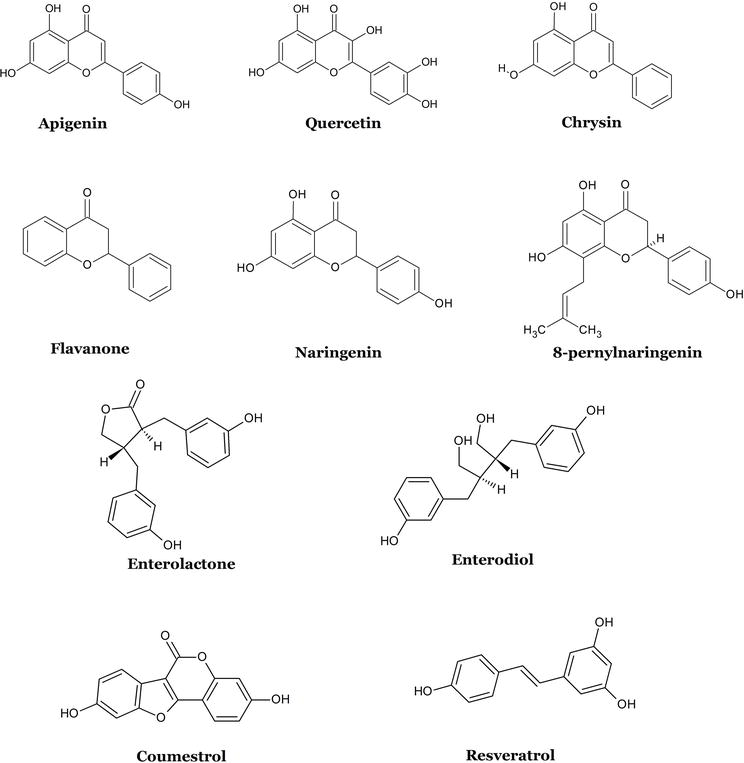
Figure 2.
Some important members of different classes of phytoestrogens [
Naturally occurring phenolic compounds namely phenolic acids, flavonoids, tannins, quinones, anthocyanins, and others play an important part in cancer prevention and/or treatment [47]. These phenolic compounds are ubiquitous and rich in medicinal herbs and dietary plants. Several phenolic compounds contribute toward inhibiting carcinogenesis mechanism and show chemopreventive activities by their diverse range of biological activities [62] (Table 4).
Advertisement
7. Herbal products used for treatment of breast cancer
A recent population-based survey showed that almost 80% of the women suffering from breast cancer use some form of complementary or alternative medicine for the treatment of cancer [63]. Herbal remedies are the well-nigh common and popular form of alternative medicine among them, which is ofttimes used past women suffering from breast cancer. Here is some evidence that can help to treat breast cancer and its associated toxicity:
7.1 Choosing a selectively cytotoxic herbal cure
One of the interesting features for herbal remedies is their selective toxicity toward cancer cells. There are a number of phytocompounds reported that have selective toxicity toward breast cancer cells. Artemisinin is ane among them, isolated from
Table 3.
Establish-based cancer therapeutics in different stages of clinical trials and enquiry [68].
7.2 Combination therapy past herbal remedies and synthetic drugs
Combination therapy of herbal therapy and constructed drugs perhaps be the final resource for patients in the terminal stage of breast cancer, where surgery is not possible [69]. The combinatory effect of a herbal drug with conventional cancer drugs might meliorate the bioavailability of i of them making the handling more effective [69, 70]. Additionally, the combinatory use of herbal remedies with chemotherapy will reduce the dose of standard medicine resulting in lower toxicity and side effects [71]. Several researchers have suggested that herbal compounds tin be used in a therapeutic modality equally it enhances the anticancer activeness of current drugs. Curcumin, a renowned anticancer herbal compound down-regulated the expression of breast cancer markers
7.3 Herbal supplements and nutraceuticals for breast cancer therapy
Cancer has been shown to be a preventable disease with changes in nutrition and dietary changes. A previous investigation showed that near 35% of cancers are related to diet [75]. There are several confirmations from epidemiological and laboratory studies that sufficient intake of fruit, vegetables, and herbal supplements is inversely linked with chest cancer occurrence. A diet composed of acceptable quantity of phytoestrogens, polyphenols, and rich sources of other chemopreventive agents helps in reducing breast cancer risk. Dietary supplements of the herbal source are less toxic and easily metabolized. Besides, dietary consumption of these herbal remedies helps in fighting side effects in postchemotherapy patients. 1 of the primary symptoms of adjuvant chemotherapeutic damage in posttherapy breast cancer patients is hot flushes. Black cohosh or
Ad
viii. Molecular mechanism of anticancerous activity of herbal compounds on chest cancer
As discussed in the before section, herbal compounds show a verity of anticancer actions—including antioxidant, cytotoxic, antiproliferative, apoptotic activity, etc. Institute-based cancer agents broadly classified into v groups that include—methyltranferase inhibitors, Dna protecting agents, antioxidants, histone deacetylases inhibitors, and mitosis disruptors. Generally, constitute-derived compounds contribute toward the anticarcinogenesis mechanism by their antioxidant, cytotoxic, antimitotic, and apoptotic activity (Tabular array 4). Others help in chemoprevention by preventing DNA damage, modulating carcinogenesis signaling, and inducing apoptotic jail cell death (Table 4). Several
Tabular array four.
Some novel compounds from herbal sources that showed promising anticancerous activity in both
8.1 Antioxidant activity of herbal compounds
Antioxidant activity of herbal compounds of oxidative stress is developed when the residue between the production of reactive oxygen species (free radicals) and antioxidant defence is disturbed [77]. Oxidative stress development and consequent reactive oxygen species (ROS) generation are linked with several disease pathogenesis including cancer. Oxidative stress is dealt with by the body'southward antioxidant machinery and several herbal compounds help boosting this machinery. For instance, curcumin enhances the activity of antioxidant enzymes resulting in enhanced cellular resistance to oxidative damage [78]. In improver, curcumin was also institute to rise hepatic GSH, SOD, GPx, GR, GST, and CAT activities in paracetamol-treated rats [79]. Other plant-based compounds similar epigallocatechin gallate, a component of in dark-green tea, plant to reduce the levels of lipid peroxidation and protein carbonyl content in rats, maybe by enhancing the GSH redox status significantly when administered orally [80]. As well, several herbal compounds assist to reduce oxidative stress, hence play a preventive function confronting cancer onset.
eight.ii Anti-angiogenesis activity of herbal compounds
Quite a few herbal compounds help to inhibit angiogenesis in breast cancer. Genistein, a flavonoid phytoestrogen, is the near potent angiogenesis inhibitor linked with reduced expression of VEGF, PDGF, uPA, and MMP-2 and MMP-ix [81]. Curcumin was even found to exist an effective inhibitor of angiogenesis that reduces the expression of various proangiogenic proteins such every bit vascular endothelial growth factor (VEGF) and bones fibroblast growth factor [82]. Resveratrol and quercetin inhibited the migration and tube formation in bovine aorta endothelial cells consequently inhibiting angiogenesis in those cells [83, 84]. In addition, catechin derivatives, such as epicatechin (EC), epigallocatechin (EGC), epicatechin-3-gallate (ECG), and epigallocatechin-3-gallate (EGCG), present in green tea are potent angiogenesis inhibitors [85]. The anti-angiogenic action of EGCG was demonstrated by inhibition of vascular endothelial growth gene (VEGF) product and reduction of matrix metalloproteinase-two (MMP-ii) activity in MDA-MB231 breast cancer cells [85].
8.3 Apoptosis-inducing activity of herbal compounds
The apoptosis-inducing activeness of herbal compounds is another favorable feature that contributes toward their anticancer consequence. Curcumin was found to inhibit the proliferation and inducing apoptosis in several cancer cell lines including chest cancer cells such every bit T47D, MCF7, MDA-MB-231, and MDA-MB-468 [115]. Curcumin inhibited the phosphorylation of protein kinase B (Akt)/mammalian target of rapamycin (mTOR), decreased BCL2 expression, and elevated BAX expression and cleavage of caspase 3, subsequently inducing apoptosis of chest cancer cells [115]. Protocatechuic acrid was also found to be a potent apoptosis inducer in 5 types of human cancer prison cell lines including chest, lung, liver, neck, and prostate cancer cells [111], which was confirmed past Deoxyribonucleic acid fragmentation, changes in mitochondrial membrane potential, and measurement of caspase activity. The flavonoid 8-prenylnaringenin (8PN), a elective of
Interestingly, artemisinin, which is an ancient Chinese herbal compound for malarial fevers, has been recently establish to have strong and selective toxicity against cancer cells. It reacts with iron to form free radicals with alkylating chapters that tin impale cells. Equally cancer cells require a large quantity of iron uptake to proliferate, making them more susceptible to the cytotoxic event of artemisinin [117]. Too, oral administration of artemisinin delayed the onset of breast cancer in 7, 12-dimethylbenz [a] anthracene (DMBA)-induced rats [118]. This encouraging results might lead to design novel chemotherapeutics with constructive anticancer belongings and low toxicity.
Advertisement
nine. Determination
Though, advances in healthcare research lead to the identification and characterization of most breast cancer types and corresponding cure. However, incidence and prevalence of breast cancer is rising in terrifying charge per unit in both adult and developing countries because of various adventure factors. Improved synthetic drugs and hormonal therapy emerged in a decline in breast cancer incidences, increased survival, and better life quality. Yet, prolonged utilise of constructed anticancer drugs is linked with several health risks or side effects that event from the toxic upshot of these drugs in normal cells. Chemoprevention past herbal compounds is of great involvement and is considered to be an inexpensive, readily applicable, adequate, and accessible arroyo to cancer control and management. Herbal remedies play a pregnant office in the management of breast cancer and the associated therapeutic toxicity. The adjunct use of herbal products and chemotherapy can be an efficient and toll-effective way to treat breast cancer. Such adjuvant therapy proved to produce a synergistic anticancer consequence that reduced the drug toxicity, suppresses drug resistance, and provides quick drug action enhancing the quality of treatment. Besides, combinatory therapy might also increase the therapeutic index of the synthetic partner by improving the efficiency of the drug. Plant-derived anticancer drugs such as vinblastine, vincristine, taxols, etc. showed encouraging chemotherapeutic potential that is currently used in chest cancer treatment and a large number of them are in preclinical or in clinical trials. In the last decade, a vast number of phytochemicals were identified that showed encouraging anticancer activity
References
- ane.
Lukong KE. Understanding breast cancer – The long and winding road. BBA Clinical. 2017; 7 :64-77 - 2.
Hennessy BT, Gonzalez-Angulo AM, Carey MS, Mills GB. A systems approach to analysis of molecular complexity in breast cancer. Clinical Cancer Research. 2009; 15 (2):417-419 - 3.
Caffarel MM, Pensa Due south, Wickenden JA, Watson CJ. Molecular biology of breast cancer. In: eLS. Chichester, UK: John Wiley & Sons, Ltd; 2016. pp. i-ix - 4.
Shareef M, Ashraf MA, Sarfraz M. Natural cures for chest cancer treatment. Saudi Pharmaceutical Journal. 2016; 24 (3):233-240 - five.
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a Cancer Journal for Clinicians. 2018; 68 (6):394-424 - 6.
Ferlay J et al. Global Cancer Observatory: Cancer Today. Lyon, France: International Bureau for Inquiry on Cancer. Bachelor from : https://gco.iarc.fr/today ; 2018 - 7.
Rice S, Whitehead SA. Phytoestrogens and breast cancer - promoters or protectors? Endocrine-Related Cancer. 2006; xiii (4):995-1015 - eight.
Anand P et al. Cancer is a preventable affliction that requires major lifestyle changes. Pharmaceutical Research. 2008; 25 (9):2097-2116 - 9.
Lambertini M et al. Reproductive behaviors and risk of developing chest cancer co-ordinate to tumor subtype: A systematic review and meta-assay of epidemiological studies. Cancer Treatment Reviews. 2016; 49 :65-76 - 10.
Mørch LS, Skovlund CW, Hannaford PC, Iversen L, Fielding S, Lidegaard Ø. Contemporary hormonal contraception and the risk of chest cancer. The New England Journal of Medicine. 2017; 377 (23):2228-2239 - 11.
Hanahan D, Weinberg RA. Hallmarks of cancer: The next generation. Cell. 2011; 144 (v):646-674 - 12.
Lin W, Karin M, Lin Due west, Karin 1000. A cytokine-mediated link between innate amnesty, inflammation, and cancer find the latest version: Review series a cytokine-mediated link between innate immunity, inflammation, and cancer. The Journal of Clinical Investigation. 2007; 117 (five):1175-1183 - 13.
Harris TJR, McCormick F. The molecular pathology of cancer. Nature Reviews. Clinical Oncology. 2010; 7 :251-265 - xiv.
Wickenden JA, Watson CJ. Key signalling nodes in mammary gland development and cancer. Signalling downstream of PI3 kinase in mammary epithelium: A play in 3 Akts. Chest Cancer Research. 2010; 12 (two):202 - 15.
Dayem AA, Choi HY, Yang GM, Kim K, Saha SK, Cho SG. The anti-cancer effect of polyphenols against breast cancer and cancer stem cells: Molecular mechanisms. Nutrients. 2016; 8 (nine) - xvi.
Fresco P, Borges F, Diniz C, Marques MPM. New insights on the anticancer properties of dietary polyphenols. Medicinal Research Reviews. 2006; 26 :747-766 - 17.
Davies E, Hiscox S. New therapeutic approaches in breast cancer. Maturitas. 2011; 68 (2):121-128 - 18.
Howell A. The endocrine prevention of chest cancer. All-time Practise & Enquiry. Clinical Endocrinology & Metabolism. 2008; 22 (four):615-623 - 19.
Bright EE, Petrie KJ, Partridge AH, Stanton AL. Barriers to and facilitative processes of endocrine therapy adherence amidst women with breast cancer. Breast Cancer Research and Treatment. 2016; 158 (two):243-251 - 20.
Tjan-Heijnen VCG et al. Extended adjuvant aromatase inhibition after sequential endocrine therapy (DATA): A randomised, phase 3 trial. The Lancet Oncology. 2017; xviii (11):1502-1511 - 21.
Venturini M, Del Mastro L. Condom of adjuvant aromatase inhibitor therapy. Cancer Treatment Reviews. 2006; 32 (7):548-556 - 22.
Masuda H, Zhang D, Bartholomeusz C, Doihara H, Hortobagyi GN, Ueno NT. Role of epidermal growth factor receptor in breast cancer. Chest Cancer Inquiry and Treatment. 2012; 136 (two):331-345 - 23.
Costa R et al. Targeting epidermal growth factor receptor in triple negative chest cancer: New discoveries and practical insights for drug development. Cancer Treatment Reviews. 2017; 53 (2017):111-119 - 24.
Chen T, Sun Y, Ji P, Kopetz Due south, Zhang W. Topoisomerase IIα in chromosome instability and personalized cancer therapy. Oncogene. 2015; 34 (31):4019-4031 - 25.
Van Vuuren RJ, Visagie MH, Theron AE, Joubert AM. Antimitotic drugs in the treatment of cancer. Cancer Chemotherapy and Pharmacology. 2015; 76 (6):1101-1112 - 26.
Lo EJ et al. DrugBank v.0: A major update to the drug bank database for 2018. Nucleic Acids Enquiry. 2017. Available from: https://world wide web.drugbank.ca/ - 27.
Middleton J, Stover D, Hai T. Chemotherapy-exacerbated breast cancer metastasis: A paradox explainable by dysregulated adaptive-response. International Journal of Molecular Sciences. 2018; 19 (11):3333 - 28.
Tao JJ, Visvanathan Grand, Wolff Air-conditioning. Long term side effects of adjuvant chemotherapy in patients with early chest cancer. The Breast. 2015; 24 (3):S149-S153 - 29.
50 SC, Abram R. Side effects of adjuvant handling of breast cancer. The New England Journal of Medicine. 2001; 344 :1997-2008 - 30.
Partridge AH, Burstein HJ, Winer EP. Side effects of chemotherapy and combined chemohormonal therapy in women with early-stage breast cancer. Journal of the National Cancer Institute. Monographs. 2001; 2001 :135-142 - 31.
N. P. Staff, Grisold A, Grisold W, Windebank AJ. Chemotherapy-induced peripheral neuropathy: A current review. Annals of Neurology. 2017; 81 (vi):772-781 - 32.
Galluzzi L, Buqué A, Kepp O, Zitvogel L, Kroemer 1000. Immunogenic prison cell decease in cancer and communicable diseases. Nature Reviews. Immunology. 2017; 17 (two):97-111 - 33.
Vassilakopoulou M, Boostandoost Eastward, Papaxoinis One thousand, de La Motte Rouge T, Khayat D, Psyrri A. Anticancer treatment and fertility: Effect of therapeutic modalities on reproductive arrangement and functions. Critical Reviews in Oncology/Hematology. 2016; 97 (2015):328-334 - 34.
Blumenfeld Z. Chemotherapy and fertility. All-time Practice & Research. Clinical Obstetrics & Gynaecology. 2012; 26 (three):379-390 - 35.
U. Department of Health, H. Services, North. Institutes of Health Osteoporosis, and R. Bone Diseases National Resource Middle. What People Chest Cancer Survivors Need To Know Virtually Osteoporosis. NIH Publication No: 18-7898. 2018. p. 1-iii. Available from: https://www.basic.nih.gov/ - 36.
Chang H-M, Moudgil R, Scarabelli T, Okwuosa TM, Yeh ETH. Cardiovascular complications of cancer therapy. Periodical of the American College of Cardiology. 2017; lxx (20):2536-2551 - 37.
Keilani Thousand, Hasenoehrl T, Neubauer One thousand, Crevenna R. Resistance exercise and secondary lymphedema in breast cancer survivors—A systematic review. Supportive Care in Cancer. 2016; 24 (4):1907-1916 - 38.
Fadol AP. Management of chemotherapy-induced left ventricular dysfunction and heart failure in patients with cancer while undergoing cancer handling: The Doc Anderson practise. Frontiers in Cardiovascular Medicine. 2018; 5 (March):one-v - 39.
Pinder MC, Duan Z, Goodwin JS, Hortobagyi GN, Giordano SH. Congestive heart failure in older women treated with adjuvant anthracycline chemotherapy for breast cancer. Journal of Clinical Oncology. 2007; 25 (25):3808-3815 - 40.
Swain SM, Whaley FS, Ewer MS. Congestive heart failure in patients treated with doxorubicin: A retrospective analysis of three trials. Cancer. 2003; 97 (11):2869-2879 - 41.
Mitry MA, Edwards JG. Doxorubicin induced middle failure: Phenotype and molecular mechanisms. IJC Heart & Vasculature. 2016; 10 :17-24 - 42.
Wolff Air-conditioning et al. Risk of marrow neoplasms after adjuvant breast cancer therapy: The national comprehensive cancer network experien. Periodical of Clinical Oncology. 2015; 33 :340-348 - 43.
Hwang KH, Cho OH, Yoo YS. Symptom clusters of ovarian cancer patients undergoing chemotherapy, and their emotional status and quality of life. European Journal of Oncology Nursing. 2016; 21 :215-222 - 44.
Ahmad SS, Reinius MA, Hatcher HM, Ajithkumar Tv. Anticancer chemotherapy in teenagers and young adults: Managing long term side effects. BMJ. 2016; 354 :i4567 - 45.
Weinberg SE, Chandel NS. Targeting mitochondria metabolism for cancer therapy. Nature Chemic Biology. 2015; eleven (ane):9-xv - 46.
Yuan H, Ma Q , Ye L, Piao G. The traditional medicine and modern medicine from natural products. Molecules. 2016; 21 (5):559 - 47.
Huang WY, Cai YZ, Zhang Y. Natural phenolic compounds from medicinal herbs and dietary plants: Potential use for cancer prevention. Diet and Cancer. 2010; 62 :1-20 - 48.
Amaral RG. Natural products as handling against cancer: A historical and electric current vision. Clinical Oncology. 2019; iv, 2018 (Jan):one-5 - 49.
Zyad A, Leouifoudi I, Tilaoui 1000, Mouse HA, Khouchani M, Jaafari A. Natural products every bit cytotoxic agents in chemotherapy against cancer. In: Cytotoxicity. Vol. i. Rijeka: InTechOpen; 2018. p. thirteen - fifty.
Howell A et al. Chance determination and prevention of chest cancer. Breast Cancer Inquiry. 2014; 16 (5):446 - 51.
Samavat H, Kurzer MS. Estrogen metabolism and breast cancer. Cancer Messages. 2015; 356 (two):231-243 - 52.
Orlando L et al. Molecularly targeted endocrine therapies for breast cancer. Cancer Treatment Reviews. 2010; 36 (Suppl 3):S67-S71 - 53.
Lamartiniere CA. Protection against breast cancer with genistein: A component of soy. The American Journal of Clinical Diet. 2000; 71 (vi):1705S-1707S - 54.
Russo M et al. Understanding genistein in cancer: The 'adept' and the 'bad' effects: A review. Nutrient Chemistry. 2016; 196 (March):589-600 - 55.
Zhao E, Mu Q. Phytoestrogen biological actions on mammalian reproductive organization and cancer growth. Scientia Pharmaceutica. 2011; 79 (one):i-20 - 56.
Alexander South. Phytoestrogens and their effects. European Periodical of Pharmacology. 2014; 741 :230-236 - 57.
Rietjens IMCM, Louisse J, Beekmann Grand. The potential health effects of dietary phytoestrogens. British Journal of Pharmacology. 2017; 174 (11):1263-1280 - 58.
de Kleijn MJJ et al. Intake of dietary phytoestrogens is depression in postmenopausal women in the United states: The Framingham study. The Journal of Nutrition. 2018; 131 :1826-1832 - 59.
Molina 50, Bustamante FA, Bhoola KD, Figueroa CD, Ehrenfeld P. Possible role of phytoestrogens in breast cancer via GPER-1/GPR30 signaling. Clinical Scientific discipline. 2018; 132 (24):2583-2598 - lx.
Ziegler RG. Phytoestrogens and breast cancer. The American Journal of Clinical Nutrition. 2004; 79 (2):183-184 - 61.
Kim Southward et al. PubChem 2022 update: Improved admission to chemical data. Nucleic Acids Research. 2019; 47 (D1):D1102-D1109 - 62.
Ambriz-Perez DL, Leyva-Lopez N, Gutierrez-Grijalva EP, Heredia JB. Phenolic compounds: Natural alternative in inflammation treatment. A review. Cogent Food & Agronomics. 2016; two (1):1-14 - 63.
Johnson SB, Park HS, Gross CP, Yu JB. Use of culling medicine for cancer and its bear upon on survival. Periodical of the National Cancer Institute (JNCI). 2018; 110 (1):121-124 - 64.
Singh NP, Lai H. Selective toxicity of dihydroartemisinin and holotransferrin toward human breast cancer cells. Life Sciences. 2001; 70 :49-56 - 65.
Ko YS et al. Polyphenols from Artemisia annua Fifty inhibit adhesion and EMT of highly metastatic breast cancer cells MDA-MB-231. Phytotherapy Research. 2016;30 :1180-1188 - 66.
Khaghani S, Razi F, Yajloo MM, Paknejad M, Shariftabrizi A, Pasalar P. Selective cytotoxicity and apoptogenic activity of Hibiscus sabdariffa aqueous extract confronting MCF-7 human breast cancer cell line. Periodical of Cancer Therapy. 2011;02 (03):394-400 - 67.
Gao H et al. Tumor cell selective cytotoxicity and apoptosis induction by an herbal grooming from Brucea javanica . North American Journal of Medical Sciences (Boston). 2011;iv (2):62-66 - 68.
Wishart DS et al. DrugBank 5.0: A major update to the DrugBank database for 2018. Nucleic Acids Research. 2018; 46 (D1):D1074-D1082 - 69.
Efferth T et al. Integration of phytochemicals and phytotherapy into cancer precision medicine. Oncotarget. 2017; 8 (30):50284-50304 - lxx.
Mangla B, Kohli K. Combination of natural amanuensis with constructed drug for the breast cancer therapy. International Journal of Drug Development and Research. 2009; 10 (1):22-26 - 71.
Patwardhan B, Vaidya ADB. Natural products drug discovery: Accelerating the clinical candidate development using reverse pharmacology approaches. Indian Journal of Experimental Biology. 2010; 48 (three):220-227 - 72.
Royt Thousand, Mukherjee S, Sarkar R, Biswas J. Curcumin sensitizes chemotherapeutic drugs via modulation of PKC, telomerase, NF-kappaB and HDAC in breast cancer. Therapeutic Delivery. 2011; 2 (10):1275-1293 - 73.
Zhan Y, Chen Y, Liu R, Zhang H, Zhang Y. Potentiation of paclitaxel activity past curcumin in human breast cancer cell by modulating apoptosis and inhibiting EGFR signaling. Archives of Pharmacal Research. 2014; 37 (8):1086-1095 - 74.
Yu Y, Zhou Q , Hang Y, Bu X, Jia West. Antiestrogenic issue of 20S-protopanaxadiol and its synergy with tamoxifen on breast cancer cells. Cancer. 2007; 109 (11):2374-2382 - 75.
Doll R, Peto R. The causes of cancer: Quantitative estimates of avoidable risks of cancer in the Usa today. Journal of the National Cancer Institute. 1981; 66 (half-dozen):1191-1308 - 76.
Roberts H. Safe of herbal medicinal products in women with breast cancer. Maturitas. 2010; 66 :363-369 - 77.
Poprac P, Jomova K, Simunkova One thousand, Kollar V, Rhodes CJ, Valko Chiliad. Targeting free radicals in oxidative stress-related human diseases. Trends in Pharmacological Sciences. 2017; 38 (seven):592-607 - 78.
Motterlini R, Foresti R, Bassi R, Green CJ. Curcumin, an antioxidant and anti-inflammatory agent, induces heme oxygenase-ane and protects endothelial cells against oxidative stress. Complimentary Radical Biology & Medicine. 2000; 28 (8):1303-1312 - 79.
Farghaly HS, Hussein MA. Protective upshot of curcumin against paracetamol-induced liver damage. Australian Journal of Basic and Applied Sciences. 2010; 4 (ix):4266-4274 - lxxx.
Kumaran VS, Arulmathi Chiliad, Srividhya R. Repletion of antioxidant condition by EGCG and retardation of oxidative damage induced macromolecular anomalies in anile rats. Experimental Gerontology. 2008; 43 :176-183 - 81.
Pratheeshkumar P et al. Cancer prevention with promising natural products: Mechanisms of activity and molecular targets. Anti-Cancer Agents in Medicinal Chemistry. 2012; 12 (10):1159-1184 - 82.
Fu Z, Chen X, Guan S, Yan Y, Lin H, Hua Z-C. Curcumin inhibits angiogenesis and improves defective hematopoiesis induced by tumor-derived VEGF in tumor model through modulating VEGF-VEGFR2 signaling pathway. Oncotarget. 2015; half-dozen (23):19469-19482 - 83.
Singh CK, Chhabra G, Ahmad North. Resveratrol and cancer cell biology. In: Resveratrol: State-of-the-Fine art Science and Health Applications. World Scientific; 2018. pp. 183-207 - 84.
Balakrishnan S et al. Golden nanoparticle-conjugated quercetin inhibits epithelial-mesenchymal transition, angiogenesis and invasiveness via EGFR/VEGFR-2-mediated pathway in breast cancer. Cell Proliferation. 2016; 49 (6):678-697 - 85.
Wang Z et al. Broad targeting of angiogenesis for cancer prevention and therapy. Seminars in Cancer Biology. 2015; 35 :S224-S243 - 86.
Liu P et al. Anti-cancer activities of allyl isothiocyanate and its conjugated silicon quantum dots. Scientific Reports. 2018; 8 (1):1-xi - 87.
Geng F et al. Allyl isothiocyanate arrests cancer cells in mitosis, and mitotic arrest in turn leads to apoptosis via Bcl-2 poly peptide phosphorylation. The Journal of Biological Chemistry. 2011; 286 :32259-32267 - 88.
Slezakova S, Ruda-kucerova J. Anticancer activity of artemisinin and its derivatives. Anticancer Enquiry. 2017; 37 (11):5995-6003 - 89.
Tin Every bit, Sundar SN, Tran KQ , Park AH, Poindexter KM, Firestone GL. Antiproliferative effects of artemisinin on human chest cancer cells requires the downregulated expression of the E2F1 transcription cistron and loss of E2F1-target cell wheel genes. Anti-Cancer Drugs. 2012; 23 (iv):370-379 - 90.
Moon YJ, Shin BS, An Grand, Morris ME. Biochanin a inhibits breast cancer tumor growth in a murine xenograft model. Pharmaceutical Research. 2008; 25 :2158-2163 - 91.
Bhushan A, Sehdev V, Lai JCK. Biochanin a modulates cell viability, invasion, and growth promoting signaling pathways in HER-2-positive breast cancer cells. Periodical of Oncology. 2009; 2009 - 92.
Kishore Fifty, Kaur North, Singh R. Bacosine isolated from aerial parts of Bacopa monnieri improves the neuronal dysfunction in Streptozotocin-induced diabetic neuropathy. Journal of Functional Foods. 2017; 34 ;237-247 - 93.
Mishra SR, Yadav PK, Nandhakumar P, Saini M, Kumar A, Kataria M. In vitro analysis of Bacosine as novel therapeutic agent for murine breast cancer. Proceedings of the National University of Sciences, India Section B. 2019; 89 (2):511-515 - 94.
Liu D, Chen Z. The event of curcumin on chest cancer cells. Journal of Chest Cancer. 2013; 16 (ii):133-137 - 95.
Aggarwal BB et al. Curcumin suppresses the paclitaxel-induced nuclear factor-κB pathway in breast cancer cells and inhibits lung metastasis of human breast cancer in nude mice. Clinical Cancer Research. 2005; eleven (20):7490-7498 - 96.
Choudhuri T, Pal South, Agwarwal ML, Das T, Sa G. Curcumin induces apoptosis in human breast cancer cells through p53-dependent Bax consecration. FEBS Letters. 2002; 512 (ane-three):334-340 - 97.
Hou DX, Tong X, Terahara N, Luo D, Fujii M. Delphinidin 3-sambubioside, a hibiscus anthocyanin, induces apoptosis in human leukemia cells through reactive oxygen species-mediated mitochondrial pathway. Archives of Biochemistry and Biophysics. 2005; 440 (i):101-109 - 98.
Wu CH, Huang CC, Hung CH, Yao FY, Wang CJ, Chang YC. Delphinidin-rich extracts of Hibiscus sabdariffa L. trigger mitochondria-derived autophagy and necrosis through reactive oxygen species in human being breast cancer cells. Periodical of Functional Foods. 2016; 25 :279-290 - 99.
Du GJ et al. Epigallocatechin gallate (EGCG) is the near constructive cancer chemopreventive polyphenol in green tea. Nutrients. 2012; iv (11):1679-1691 - 100.
Hong OY et al. Epigallocatechin gallate inhibits the growth of MDA-MB-231 breast cancer cells via inactivation of the β-catenin signaling pathway. Oncology Letters. 2017; fourteen (i):441-446 - 101.
Xiang LP et al. Suppressive furnishings of tea catechins on breast cancer. Nutrients. 2016; viii (viii):1-fifteen - 102.
Liggins J, Bluck LJ, Runswick S, Atkinson C, Coward WA, Bingham SA. Daidzein and genistein content of fruits and nuts. The Periodical of Nutritional Biochemistry. 2000; 11 (six):326-331 - 103.
Spagnuolo C et al. Genistein and cancer: Current status, challenges, and futurity directions. Advances in Nutrition. 2015; 6 :408-419 - 104.
Lamartiniere CA. Protection confronting breast cancer with genistein: A component. The American Periodical of Clinical Nutrition. 2018; 71 (March):1705-1707 - 105.
Cai Y, Zhao B, Liang Q , Zhang Y, Cai J, Li G. The selective effect of glycyrrhizin and glycyrrhetinic acid on topoisomerase IIα and apoptosis in combination with etoposide on triple negative breast cancer MDA-MB-231 cells. European Journal of Pharmacology. 2017; 809 (December):87-97 - 106.
Wang X-F, Zhou Q-Thousand, Lu Y-Y, Zhang H, Huang South, Su S-B. Glycyrrhetinic acid potently suppresses breast cancer invasion and metastasis by impairing the p38 MAPK-AP1 signaling axis. Proficient Opinion on Therapeutic Targets. 2015; 19 (5):577-587 - 107.
Holzapfel NP, Holzapfel BM, Champ S, Feldthusen J, Clements J, Hutmacher DW. The potential role of lycopene for the prevention and therapy of prostate cancer: From molecular mechanisms to clinical evidence. International Journal of Molecular Sciences. 2013; 14 (seven):14620-14646 - 108.
Nahum A et al. Lycopene inhibition of cell cycle progression in breast and endometrial cancer cells is associated with reduction in cyclin D levels and retentivity of p27 Kip1 in the cyclin Due east-cdk2 complexes. Oncogene. 2001; 20 (26):3428-3436 - 109.
Kakkar S, Bais S. A review on protocatechuic acid and its pharmacological potential. ISRN Pharmacology. 2014; 2014 (4):1-9 - 110.
Tseng TH et al. Inhibitory effect of hibiscus protocatechuic acid on tumor promotion in mouse skin. Cancer Letters. 1998; 126 (2):199-207 - 111.
Yin MC, Lin CC, Wu HC, Tsao SM, Hsu CK. Apoptotic effects of protocatechuic acrid in human chest, lung, liver, cervix, and prostate cancer cells: Potential mechanisms of action. Journal of Agricultural and Food Chemical science. 2009; 57 (14):6468-6473 - 112.
Woźniak Ł, Skąpska S, Marszałek One thousand. Ursolic acid - a pentacyclic triterpenoid with a broad spectrum of pharmacological activities. Molecules. 2015; 20 (xi):20614-20641 - 113.
Jäger S, Trojan H, Kopp T, Laszczyk MN, Scheffler A. Pentacyclic triterpene distribution in various plants - rich sources for a new group of multi-potent found extracts. Molecules. 2009; xiv (6):2016-2031 - 114.
Mizushina Y, Iida A, Ohta K, Sugawara F, Sakaguchi K. Novel triterpenoids inhibit both Deoxyribonucleic acid polymerase and Dna topoisomerase. The Biochemical Periodical. 2000; 350 (3):757-763 - 115.
Hu Southward, Xu Y, Meng L, Huang 50, Sun H. Curcumin inhibits proliferation and promotes apoptosis of chest cancer cells. Experimental and Therapeutic Medicine. 2018; sixteen :1266-1272 - 116.
Brunelli E, Minassi A, Appendino M, Moro L. 8-Prenylnar-ingenin, inhibits estrogen receptor-α mediated cell growth and induces apoptosis in MCF-7 breast cancer cells. The Journal of Steroid Biochemistry and Molecular Biology. 2007; 107 (iii-5):140-148 - 117.
Konstat-Korzenny E, Ascencio-Aragón J, Niezen-Lugo S, Vázquez-López R. Artemisinin and its synthetic derivatives equally a possible therapy for cancer. Medical Science. 2018; 6 (one):19 - 118.
Lai H, Singh NP. Oral artemisinin prevents and delays the evolution breast cancer in the rat. Cancer Letters. 2006; 231 :43-48
Submitted: May sixth, 2019 Reviewed: September 11th, 2019 Published: March 25th, 2020
© 2022 The Writer(south). Licensee IntechOpen. This chapter is distributed under the terms of the Creative Commons Attribution 3.0 License, which permits unrestricted use, distribution, and reproduction in whatsoever medium, provided the original work is properly cited.
Source: https://www.intechopen.com/chapters/70593
0 Response to "Which Herbal Therapies Can Be Recommended to a Client With Breast Pain? Select All That Apply."
Post a Comment